Parkinson disease
Epidemiology
Etiology
Parkinson disease
- Idiopathic
- Contributing genetic factors include:
- α-Synuclein (SNCA)
- α-Synuclein constitutes the major component of Lewy bodies. In addition to mutations, duplication/triplication of the wild-type gene can also cause PD (due to increased production of the normal protein).
- α-Synuclein (SNCA)
Pathophysiology
Mnemonic
PArkinson's Disease = doPAmine Dowm
Alzheimer Disease = Acetylcholine Down
- Progressive dopaminergic neuron degeneration in the substantia nigra (part of the basal ganglia) and the locus coeruleus → dopamine deficiency at the respective receptors of the striatum with interrupted transmission to the thalamus and motor cortex → motor symptoms of PD
- Serotonin and noradrenaline depletion (in the raphe nuclei): likely cause of depressive symptoms
- Acetylcholine surplus (in the nucleus basalis of Meynert): likely cause of dyskinesia
Clinical features
Motor signs
- Parkinsonism
- Bradykinesia: slowed movements in combination with decreased amplitude/speed when moving
- Resting tremor (4–6 Hz)
- Oftentimes the presenting symptom
- Pill-rolling tremor that subsides with voluntary movements but increases with stress
- Rigidity: increased and persistent resistance to passive joint movement that is independent of speed
- Cogwheel rigidity
- Postural instability
- Imbalance and tendency to fall
- Parkinsonian gait: shuffling gait with quickened and shortened steps
Diagnostics
Pathology
- Lewy bodies
- Aggregates of misfolded α-synuclein and other proteins, such as ubiquitin and neurofilament protein within the neural cell bodies
- Appear histologically as intracellular hyaline eosinophilic globules
- May be found in brainstem, substantia nigra, and cortex
- Also seen in Lewy body dementia
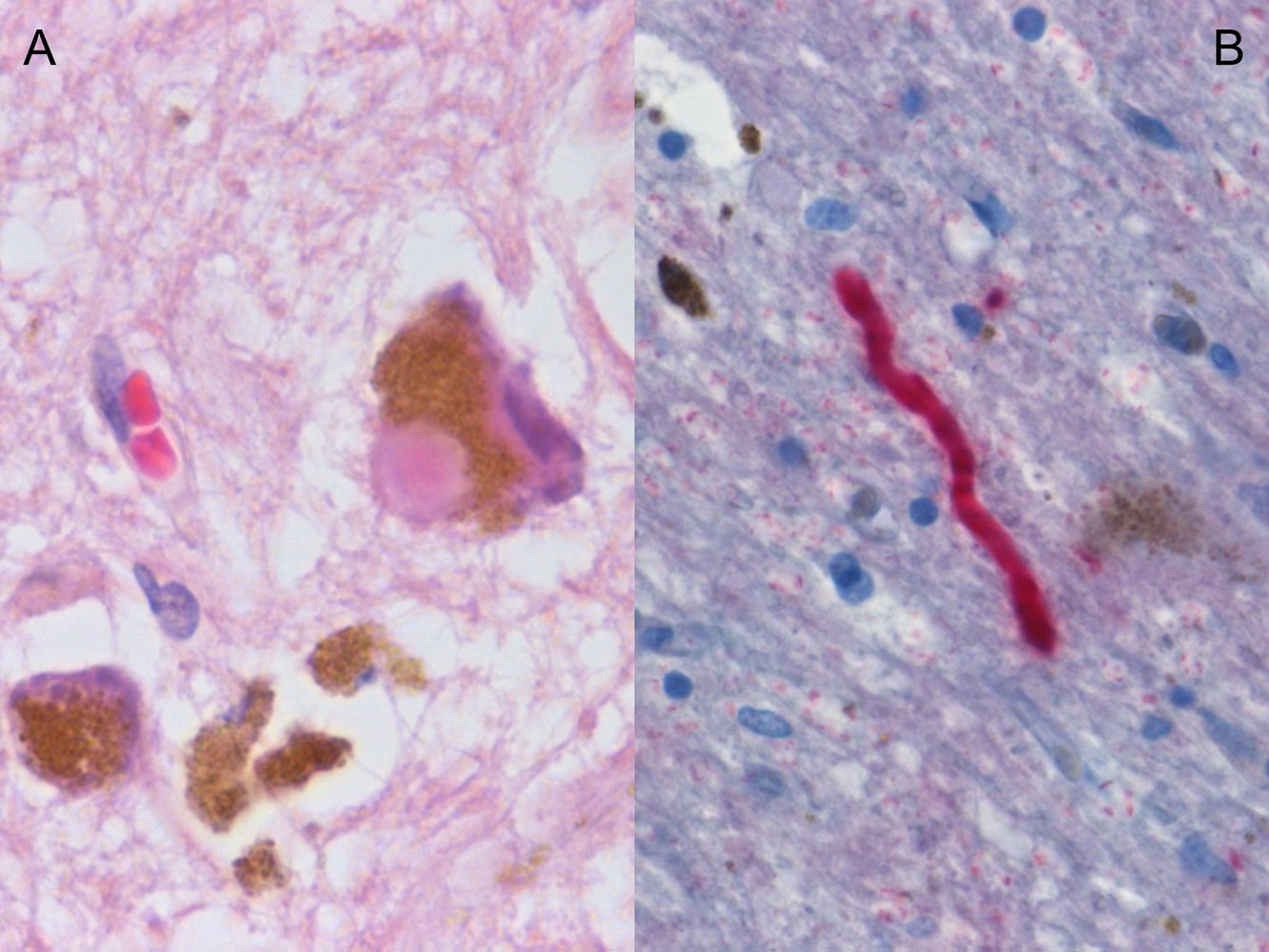
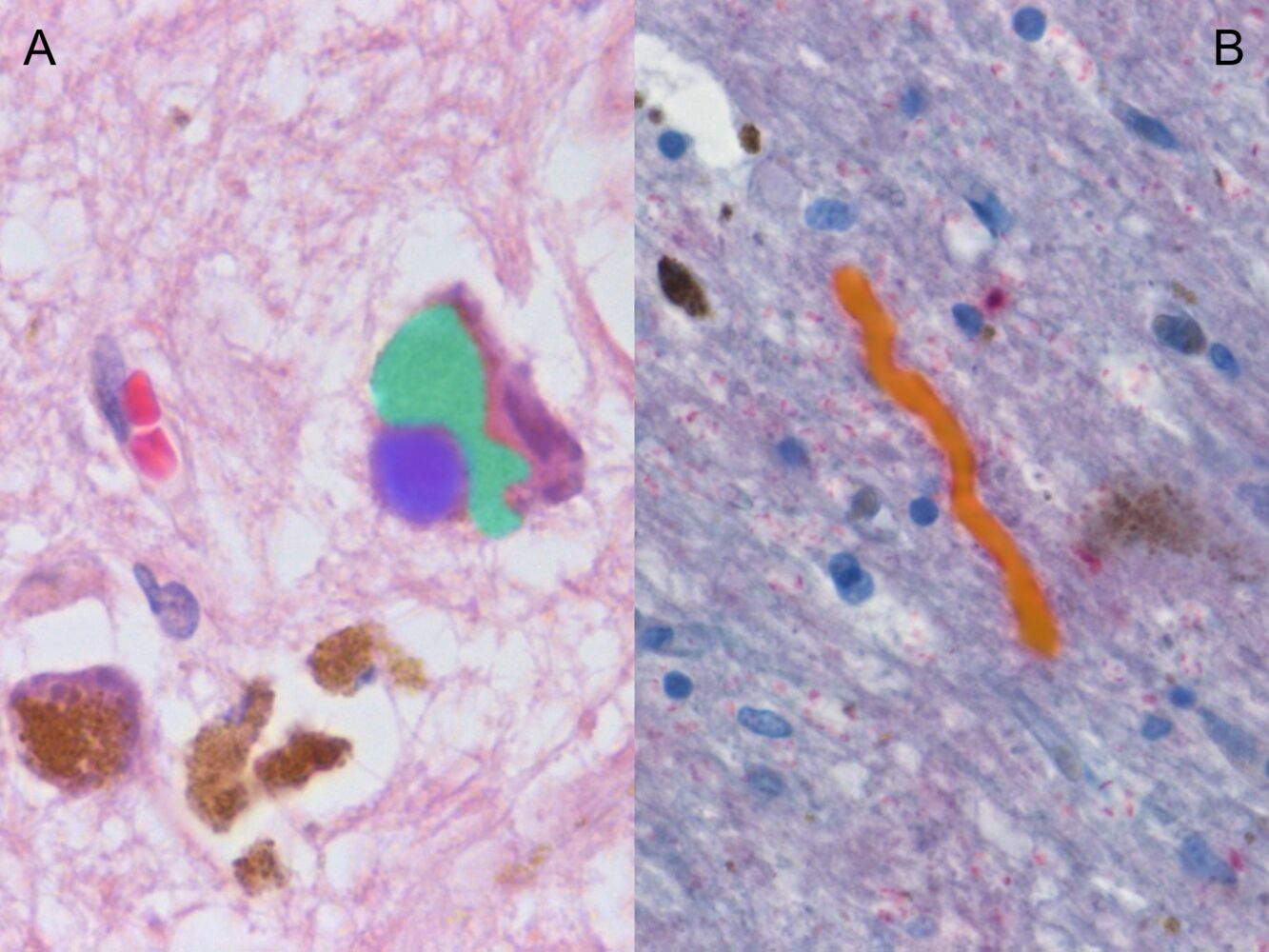
- Image A: An eosinophilic cytoplasmic inclusion (Lewy body; blue overlay) is visible inside a neuron. There is a large accumulation of neuromelanin (brown granules; green overlay).
- Image B: A neurite staining positive for α-synuclein is visible in the center of the image (Lewy neurite; yellow overlay).
Treatment
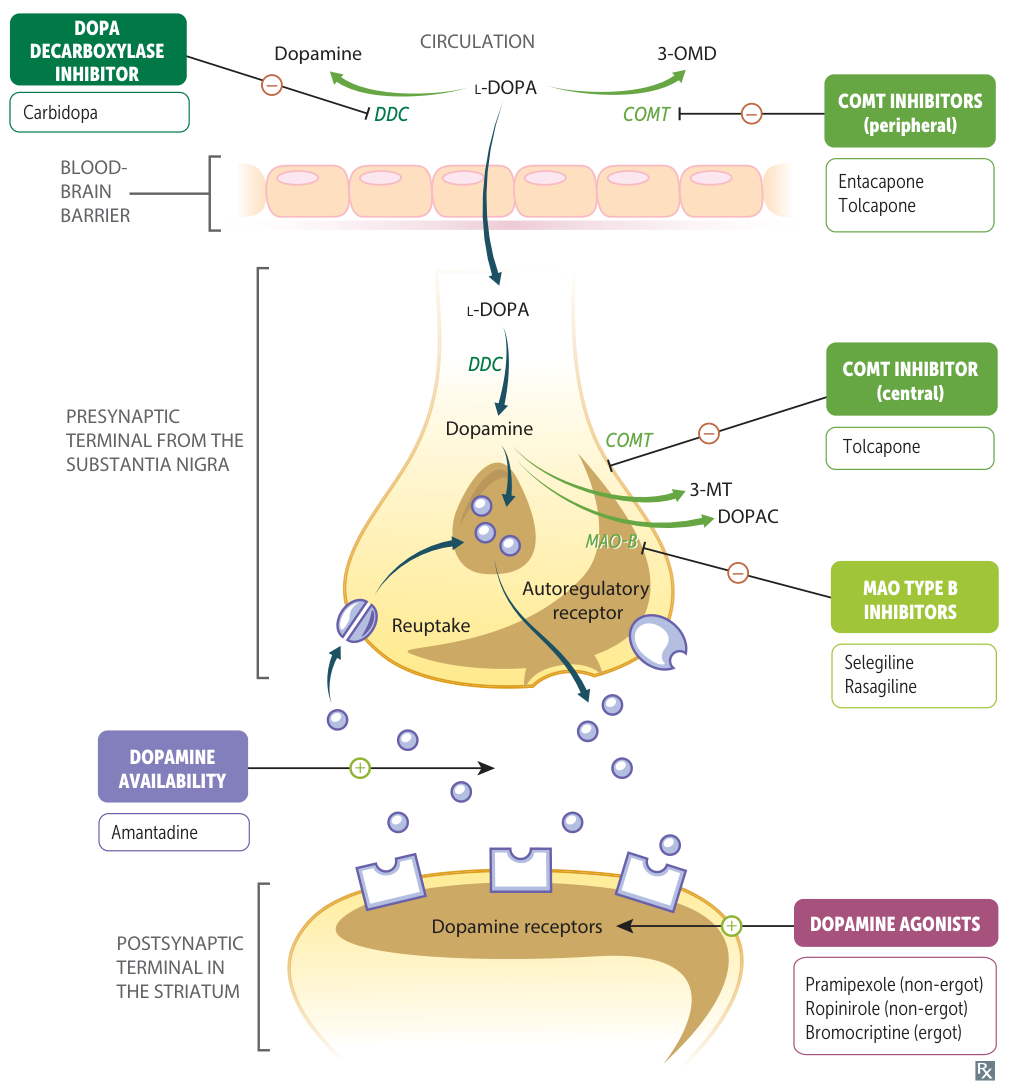
Nonergot dopamine receptor agonists
- Pramipexole, Ropinirole, Apomorphine
- Consider as initial treatment in younger patients, especially those with risk factors for levodopa-induced dyskinesia.
- Some patients develop impulse control disorders with compulsive gambling or hypersexuality.
Tip
- Ergot dopamine agonists (cabergoline and bromocriptine) are not recommended in Parkinson disease or restless leg syndrome, but are first-line treatment in Prolactinoma and Hyperprolactinemia.
- Primarily due to a higher risk of serious side effects, specifically fibrotic reactions affecting the heart valves and lungs.
- The doses used for Prolactinoma and Hyperprolactinemia are generally lower than for Parkinson's, leading to a lower risk of fibrotic side effects, making the benefit-risk balance more favorable.
Anticholinergic drugs (muscarinic antagonists)
- Benztropine, Trihexyphenidyl, Biperiden
- Beneficial regarding tremor and rigidity but does not improve bradykinesia
Deep brain stimulation (DBS)
- In PD, the lack of dopamine leads to overactivity in the indirect pathway. Key players here are the STN and the GPi.
- Indications
- Severe motor symptoms or refractory tremor
- Decrease in dosage of medication because of adverse effects
- Procedure
- Stereotactic implantation of stimulating electrode(s) targeting the subthalamic nucleus or internal globus pallidus
- Controlled remotely